Review of JFK Photographs and X-rays at the National Archives, September 23, 2004
Larry M. Sturdivan
October 2, 2004
In addition to those things that Dr. Chad Zimmerman and I were hoping to observe, there were specific questions asked by Dr. Robert Grossman and Mr. John Hunt that we tried to answer. Most of these were similar to our own objectives, but we did pay special attention to the details that were of specific interest to them. Here is my impression. Chad will do one later.
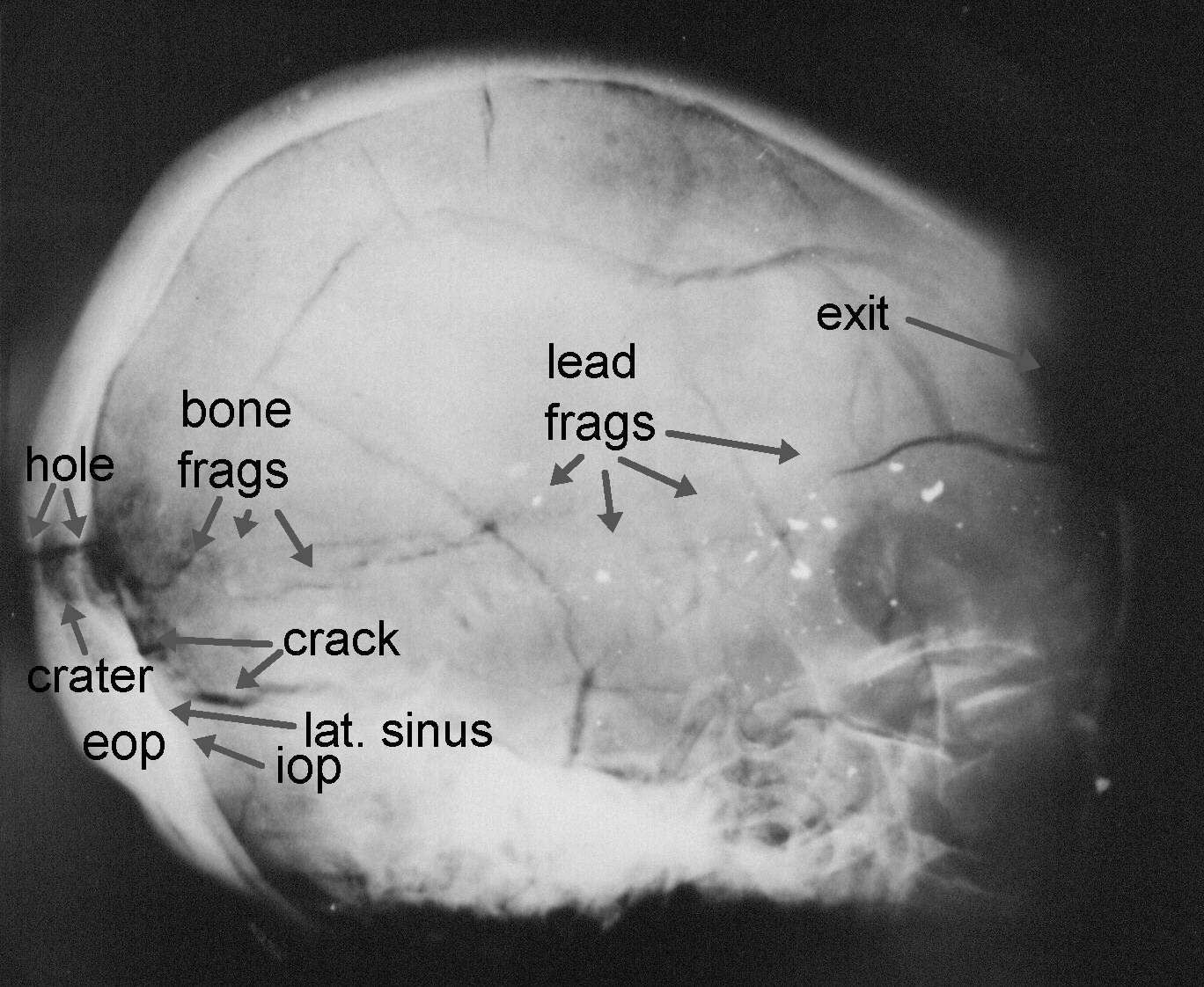
First, Dr. Grossman asked the question that is of interest to everybody: is there a crater on the interior of the back of the skull in the lateral x-ray or the enhanced version? Another thing that everybody was curious about was whether the enhanced lateral x-ray showed the entire back of the head, like the unenhanced print does. Yes, it does. However, there is no unequivocal evidence of a crater at either proposed entry point visible on either the original or the enhanced print. There is a craterlike dark area at the autopsy entry location that I would ordinarily think was an entry crater, but it is not too unlike the dark area in JFK’s life x-ray printed in the HSCA report. It might be adjacent to the lateral sinus. However, immediately behind this dark cone-shaped area there is a clearly visible dark streak across the occipital bone in the enhanced x-ray at the autopsy entry site. This streak resembles the dark path of the entry wound in one of the Biophysics x-rays of Figure 1.
Figure 1. X-ray of an Experimental Skull from the Biophysics Division Tests (one of four)
This void is within the area that is cut off in the copy of the enhanced lateral x-ray printed in the HSCA report (JFK Exhibit F-53). I don’t want to seem paranoid, but one cannot help but wonder if the released copy were deliberately cropped to eliminate this shadow. At the House Forensic Pathology Panel (FPP) entry site there is no sign of a crater or transverse hole. The only features visible at that location are the offset crack and the shadow on the exterior of the skull identified by the FPP as the lateral view of the notched disk-like shadow seen on the anterior-posterior (A-P) x-ray. (More on this later). The important point is that there is a small hole in the back of the head with bone chips just inside it. This is conclusive evidence that the entry was on the back, not the side or front.
Second, Dr. Grossman asked us to determine the angle to which the head is inclined in the lateral x-ray published in the HSCA report, Volume I. As the horizontal reference, we used the standard Frankfort plane, defined as a line from the inferior (lower) margin of the orbit through the center of the external auditory meatus (ear canal). There were two lateral x-rays, one much clearer than the other. The less clear one was also poorly centered so that a large portion of the rear of the skull was off the edge of the film. The clearer one is the one published in the report. On this original there are two pencil lines that the National Archives (NA) staff said were there when the NA acquired them (presumably at the time they were returned by Robert Kennedy). One line was parallel to the upper and lower edges of the x-ray film. A faint image of this line may be seen in the enhanced print in the report, JFK Exhibit F-53, page 240, Vol. I. The print is aligned the same way as the original, though the printed version is cropped, eliminating the lower face.
The angle between the line and the Frankfort plane is between 4.5 and 5 degrees. The uncertainty is due to the difficulty in determining the inferior margin of the orbit. This measurement is made more easily from the enhanced version. Thus, the head is tilted forward about 5 degrees in the published lateral view.
Before continuing with other questions, I will comment on the angular tilt of the A-P view. The complete A-P view has the complete face, including an arched view of the upper teeth. On the x-ray, the distance between a line across the bottom of the back teeth and the bottom of the front incisors is 7 mm. Unfortunately, I neglected to measure the span of the teeth from rear molar to front incisor on the lateral view. Assuming the typical distance of 55 mm would give an upper tilt to the dentition of about 7.5 degrees (see Figure 2). The angle between the plane of the bottom of the upper teeth and the Frankfort plane was 4°. Thus, the net upward tilt of the head in the A-P view would be 11.5°. I will ask Dr. Grossman to make an exact measurement of the span of the teeth on the lateral x-ray and will correct the estimate at that time.
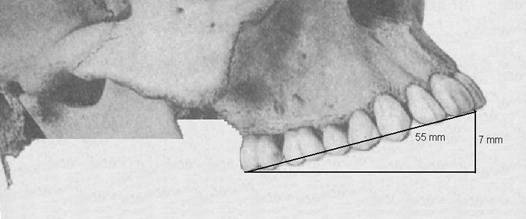
Figure 2. Angle of Dentition in JFK Anterior-Posterior X-ray
John Hunt asked several questions. The first: Can damage to the flocculus be seen in the brain photos? We examined several photos. There was no visible damage to the right cerebellum in any. The area of the flocculus on the right was obscured by the medulla and pons; as the brain was still as near intact as it was before removal.
When shown the picture of the underside of the brain, I was surprised to see a wide strip of damage to the underside of the left cerebellum, front to back. As no mention of this damage was made by any of the three pathologists and it was on the side opposite to the path of the bullet, I assumed that it was postmortem. The usual method of removing the brain for examination (as explained to me by a prominent California medical examiner) is to approach from the front, trimming the blood vessels and nerves that hold the brain to the skull and lifting the frontal lobes until the cord can be severed. Because the JFK brain was not removed through the usual skullcap orifice, but through the hole created by removing the loose bone flaps, the hole in the skull was further toward the rear than usual. Thus, the brain may have been removed with an approach from the back. In this case, the damage to the underside of the left cerebellum might have been caused when it was lifted or when a scalpel was inserted to sever the cord.
John also asked if any of the recovered fragments could be recognized on the x-rays. Disappointingly, the x-rays are not much more distinct than the released copies. I was unable to identify the fragments that were recovered. This is made difficult by the fact that the orientation of the shadows is likely quite different from the orientation of the fragments in the photographs.
One thing that I did note was that the light area identified by the FPP as the lateral view of the notched metallic disk seen at the FPP entry site on the A-P view was not nearly as bright as even the very small lead fragments. This optical density was not nearly as great as a disk-like metal object should be when viewed edge-on. Both it and the light patch visible on the frontal bone were clearly on the exterior of the skull, between skull and scalp. The optical density of these two objects was about the same as that of the bone fragments and much less bright than the metal fragments. They were likely bone. Bone fragments could have been spalled off the outer table when the skull was cracked and displaced much like glass chips are sometimes created at the cracks when a glass is shattered. I believe that the disk-like metal object seen on the A-P view is not present in either lateral x-ray. My best guess is that it’s an artifact. It isn’t unusual that artifacts appear on autopsy x-rays. Things stick to skin, especially when there’s lots of blood. These objects may fall from the skin or hair onto the autopsy table, before or after the x-ray is taken. Thus, they appear in only one view or in different locations in different views.
John asked about the damage to the back of the head in the autopsy photographs that show JFK’s upper back and back of the head. The color photographs are much better for this than the usual black and white prints that are in the bootleg photo set. The HSCA FPP entry site on the crown of the head appears to be a pale reddish patch on the scalp or a bloodstained skull. This could be the result of a split in the scalp from the explosion, abrasion of the scalp, or perhaps liver mortis in the scalp. It does not appear to be a hole through the skull. The autopsy entry site, which would be just above the small piece of what appears to be brain tissue on the hair, is not visible as the scalp is well covered by Kennedy’s thick hair. We examined several pictures, color and b&w, but I could not see any feature that looked like a hole through scalp and skull. As medical examiner, Dr. Richard Mason, said, it’s too bad that they did not clip the hair from the entry site, take a picture of the entry through the scalp, then lay back the scalp to get a clear picture of the hole in the bone. Coupled with suitable landmarks, this would have definitively pinpointed the entry site on the skull.
One of the major points of interest on my part was to see better reproductions of the interior skull photograph with the brain removed. These exceeded my expectation, thanks to Chad’s foresight in bringing a stereoscope to the Archives. The color photographs, particularly number 44, were amazingly detailed. The entry wound was well lighted and in perfect focus. The back of the skull had what looked like puddles of bloody fluid. It was bright red and did not appear to be clotted blood. Features that sat a bit higher were not covered by the fluid and were clearly visible. The only improvement one could have asked for was for another photograph with the dura stripped away from the cratered entry wound.
In the stereo image that Chad obtained, using photographs 44 and 45, the details at the back of the skull were quite visible in three dimensions. The entry hole in the dura extended upward into the skull cavity. The area below the entry wound that looks like a dark stripe in the b&w bootleg photograph was a fluid-filled channel that was distinctly lower than the surrounding features in the 3-D image. This channel is indicated in Figure 3. The most obvious channel running horizontally across the back interior of the skull is the lateral sinus. Usually, the tentorium is only split enough to allow the brain to be removed via the frontal approach or trimmed well above the lateral sinus, so that the sinus would not be exposed.
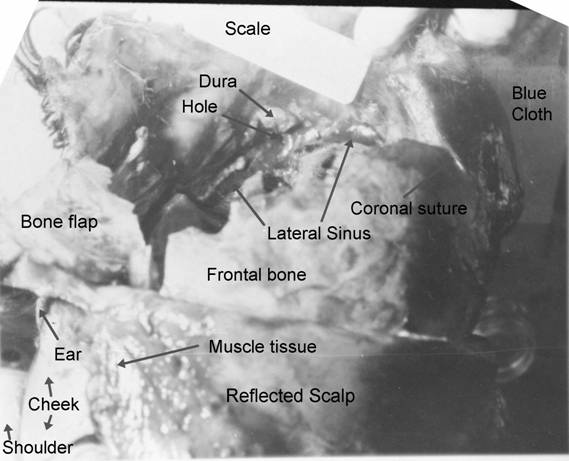
Figure 3. Photograph of Skull Interior with Annotations (see text for details)
However, if the brain was removed by approaching from the rear, as speculated above, it would have been necessary to trim the tentorium off close to the skull. In any case, this was apparently done, leaving the lateral sinus fully visible. This places the entry wound directly above the lateral sinus/tentorium, a location perfectly compatible with the massive gutter wound to the right cerebrum from the tip of the occipital lobe at the rear to the tip of the frontal lobe at the forehead. The lateral sinus is indicated in Figure 3. The line of white tissue above and below are tissue that rise a short distance into the cavity in the 3-D view. This, I believe, is the severed upper and lower attachment of the tentorium, the bifurcation of which forms the lateral sinus.
The entry hole below the puffed-up dura was nearly filled with what appeared to be a large blood clot. The clot had a hole in it that appeared nearly black, indicated in the figure. We speculated that the hole in the clot was quite deep, perhaps passing all the way through the entry hole. The interior of the skull was well lighted and had many small reflected highlights from the wet interior. All of these highlights were quite white with one exception. As implied by the fact that pictures 44 and 45 formed a stereo pair, there was an angular shift between these pictures. On #45, the inferior of the two, Chad noticed a small blue-tinged highlight at one edge of the hole through the clot in the entry crater. This highlight was the same shade of blue as the cloth on the table under the head. I agree that this highlight was likely from light reflected through the hole open all the way through the back of the skull.
The color prints had other advantages, as well. One was that the skin of the cheek was clearly discernable, as was the skin of the shoulder and ear. All had the pallor one would expect, but were clearly external. The picture numbered 44 is the only view in which a patch of exposed adipose tissue appears on the shoulder. Evidently, the autopsy team had already started to open the chest wall before this picture was taken and had folded a flap of skin from the chest back over the shoulder. The shoulder was not visible in all photographs. More of the shoulder is visible in #44 than in other, similar photographs. The underside of the reflected scalp contained a large patch of muscle fibers. From its location, I thought that it was probably from the top of the temporalis, rather than integumentary muscle.
In #44, the markings on the scale were clearly visible. As I recall, this was the only one of the pictures for which this was true. The cloudy area under the words “dura” and “hole” in Figure 3 was in neither of the color prints we examined in detail. Evidently, a stray piece of scalp was folded under the scale for this b&w shot, obscuring some of the detail in the rear of the skull. The position of the ruler in relation to the entry hole and highest portion of broken parietal bone at the top of the photograph seemed to be consistent among all exposures. None of the photographs, color or b&w, showed the specimen bottle as clearly as it is in Figure 3. Evidently, this photograph has undergone some enhancement or was taken from a print that we did not see. We were told that all prints that were in the Archives were shown to us.
One final observation was made on the x-ray of a triangular piece of bone we were shown with the other x-rays. This evidently was an x-ray of the piece of bone mentioned in the autopsy report, as containing evidence of a crater on the exterior that they thought was part of the exit wound. One side of this triangle had the unmistakable appearance of a suture; interpreted at autopsy as part of the coronal suture. This x-ray showed a number of transparent spots that were obviously small lead fragments. The Ida Dox drawing of this fragment, made for the HSCA, is shown in Figure 4 (courtesy an email from John Hunt). Chad made a similar sketch, but Miss Dox was allowed to trace directly on the x-ray, while Chad had to do a freehand sketch. Unlike the skull flaps still attached to the scalp, the lead fragments on this bone could not have been secondary deposits, stuck by clotted blood. As this fragment was dislodged in the explosion, the fragments had to be deposited into the surface of the bone by the bullet core as it punched through the skull. Note the dimensions of the fragment and extent of lead deposits, over an inch, added to the drawing. Chad and I are of the opinion that this is frontal bone. The orientation, however, is difficult to determine, as the curvature of the bone and which surface contains the crater are not determinable from the x-ray.
The gap between the two groups of lead fragments indicates that the core had probably just separated at exit. Separation of the bullet into two major pieces just before or during exit is consistent with the small angular separation of the two impact points on the windshield and trim. Lead deposits inside the cratered area indicates that the bone had already cratered before the core scraped by. This may mean that the leading surface of the bullet fragments was jacket or that the one piece of the core snapped the shelf of exterior bone before the second piece of core scraped the bone going out.
Again, this is clear evidence that the bullet entered from the back and exited at the border of the parietal and frontal bones, after the jacket had split and the lead core was exposed. Had it entered the front there would have been a small hole of entry cratered on the inside and a large exit toward the back.

Figure 4. Dox Tracing of the X-ray of a Skull Fragment Recovered from the Limousine